Members and Inclusion/Exclusion Standards
This examine retrospectively analyzed the information of feminine sufferers who underwent standardized urodynamics for decrease urinary tract signs(LUTS) in the urology division from September 2020 to March 2025 below blind evaluation. The prognosis of stress urinary incontinence (SUI) or its absence was confirmed based mostly on the urodynamic findings, adhering to the Worldwide Continence Society (ICS) definitions. A whole of 202 women with full information had been enrolled after acquiring knowledgeable consent. Amongst these, 51 had been urodynamically confirmed to have SUI, and 151 had been urodynamically confirmed to don’t have any proof of SUI or different types of urinary incontinence assembly ICS standards.
All members underwent urodynamic research (UDS) based mostly on scientific indications for evaluating decrease urinary tract signs (LUTS), together with urinary frequency (> 8 voids/day), urgency, voiding issue, or inconclusive non-invasive testing. The non-SUI management group (n = 151) consisted of women with LUTS however no urodynamic proof of SUI or different incontinence subtypes per ICS standards. Widespread diagnoses in this group included overactive bladder (34%), bladder outlet obstruction (22%), and sensory urgency (18%), all requiring UDS for differential prognosis and remedy planning.
Inclusion standards had been: (1) Feminine sufferers aged 45–80 years; (2) Full scientific information; (3) Delicate neurological issues had been permitted; and(4) No historical past of tension-free vaginal tape obturator (TVT-O) surgical procedure previous to admission.
Exclusion standards included: (1) Incomplete information; (2) Earlier historical past of any anti-incontinence surgical procedure (e.g., tension-free vaginal tape obturator [TVT-O], colposuspension, autologous fascial slings, bladder neck injections, and so forth.). or pelvic ground reconstructive surgical procedure (e.g.,anterior/posterior colporrhaphy); (3) Reasonable to extreme neurological illnesses (e.g., Alzheimer’s illness, hemiplegia, stroke); (4) Analysis of SUI and historical past of prior TVT-O surgical procedure earlier than admission; (5) Acute urinary tract an infection, urinary tumors, or different urinary emergencies; (6) Being pregnant or breastfeeding; and (7) Neurological issues (together with a number of sclerosis and peripheral neuropathy).
Moral approval was obtained from the Ethics Committee of [Blind for review]. The examine was carried out in accordance with the Declaration of Helsinki.
Knowledge Assortment and Processing
The important thing diagnostic variable, stress urinary incontinence (SUI), was outlined and decided solely based mostly on the outcomes of the standardized urodynamic analysis carried out at our establishment, which assessed for urine leakage coinciding with elevated belly strain in the absence of a detrusor contraction.
Variables had been encoded based mostly on scientific information, as proven in Desk 1.
Steady variables reminiscent of BMI and age had been categorized based mostly on clinically established thresholds to boost model interpretability and scientific utility. Particularly: BMI classifications adopted Chinese language requirements [4]: 0 = regular(18.0-23.9), 1 = chubby(24.0-27.9), 2 = overweight(≥ 28.0), as these cutoffs align with nationally acknowledged cardiometabolic risk classes. Age was dichotomized at 55 years (0: <55;1: ≥55) to mirror the established improve in SUI risk post-menopause [3]. Parity was binarized as < 3 or ≥ 3 deliveries based mostly on obstetric research indicating considerably elevated pelvic ground damage risk past two vaginal births [5]. Whereas steady variables or spline features might seize nonlinear results, these categorizations had been prioritized for three causes: (1) scientific relevance of established thresholds, (2) simplicity for nomogram implementation in routine observe, and (3) mitigation of overfitting given our pattern measurement(n = 202). Future research with bigger cohorts may discover steady parameterizations.Age (AGE) was categorized as 0 (< 55 years) or 1 (≥ 55 years). BMI classifications adopted Chinese language requirements: 0 = regular (18.0–23.9), 1 = chubby (24.0–27.9), 2 = overweight (≥ 28.0) [4]. Heavy bodily labor (JOB) was outlined as a historical past of occupations or day by day actions involving sustained heavy lifting (≥ 20 kg), extended standing (> 6 h/day), or high-intensity handbook labor (e.g., farming, building, manufacturing unit work) for ≥ 5 years, coded as 1 (current) or 0 (absent). Bodily train (PE) was outlined as Structured moderate-to-vigorous train (e.g., brisk strolling, swimming, biking, pelvic ground coaching) carried out ≥ 3 occasions/week for ≥ 30 min/session over the previous 12 months. Coded as 1 (current) or 0 (absent).Binary variables reminiscent of obstetric historical past (DG), smoking (Smoke), alcohol consumption (Alcohol), uterine surgical procedure (US), bodily train (PE), recurring consumption of tea or espresso (DL), heavy bodily labor (JOB), menopause (MP), macrosomia supply (HB), persistent constipation (CC), urethral prolapse (UP), urinary frequency (UF), diabetes (DM), hypertension (HBP), stress urinary incontinence (SUI), respiratory illnesses (BD), and urinary system illnesses (UD) had been coded as 0 (absent) or 1 (current). Stress provocative check (SP) was recorded as 0 (detrimental) or 1 (constructive), supply mode (NDM) as 0 (vaginal) or 1 (cesarean), and variety of deliveries (DT) as 0 (< 3) or 1 (≥ 3). The first consequence variable was the presence or absence of SUI.
Preliminary information preprocessing concerned eradicating data with incomplete information, ensuing in a remaining dataset of 202 sufferers. The cleaned dataset was randomly divided into coaching (roughly 151 sufferers) and validation units (roughly 51 sufferers) at a 7:3 ratio. Baseline traits for each units are introduced in Desk 2. The coaching set was used for model growth, and the validation set for unbiased model testing.
Statistical strategies
Statistical analyses had been carried out utilizing R software program. Initially, Lacking information (< 5% for all variables) had been imputed utilizing the MICE package deal in R, making use of a number of imputation with chained equations below the MAR assumption. A priori pattern measurement estimation was carried out utilizing the strategy for evaluating the AUC of a predictive model towards a null model (AUC = 0.5). Assuming an anticipated AUC of 0.75, a significance stage of 0.05, energy of 80%, and a case-control ratio of roughly 2:1, a minimal of 180 members was required. The ultimate pattern measurement of 202 met this requirement.
Candidate predictor variables had been screened utilizing Least Absolute Shrinkage and Choice Operator (LASSO) binary logistic regression in the coaching dataset. LASSO introduces a penalty time period to shrink sure regression coefficients towards zero, facilitating characteristic choice and mitigating multicollinearity, thus figuring out probably the most predictive variables for the result [6, 7]. 5-fold cross-validation was employed to pick out optimum variables on the λ worth minimizing imply squared error (Fig. 1A illustrates the LASSO regression coefficient paths, and Fig. 1B depicts model parameter choice). Subsequently, chosen variables entered a multivariable logistic regression model utilizing a ahead stepwise methodology to find out remaining predictors and their regression coefficients. Primarily based on the multivariate logistic regression model, a nomogram was developed to offer an intuitive software for individualized SUI risk evaluation (Fig. 2). The nomogram integrates six key predictors: BMI, urethral prolapse (UP), diabetes (DM), historical past of urinary tract illnesses (UD), heavy bodily labor (JOB), and variety of deliveries ≥ 3 (DT). Every predictor is assigned a rating on a degree scale (0–100). The entire factors are transformed to a predicted SUI chance (0–100%) on the underside axis. Clinicians might use this software by summing the factors for a affected person’s particular risk profile and mapping the entire to the SUI risk chance [7].

Collection of predictive variables utilizing the LASSO regression model. (A) LASSO coefficient paths of candidate variables. (B) Cross-validation plot for optimum λ choice. Be aware: Panel A illustrates the coefficient paths for the 20 candidate variables below various λ values; panel B demonstrates the number of the optimum λ via cross-validation.
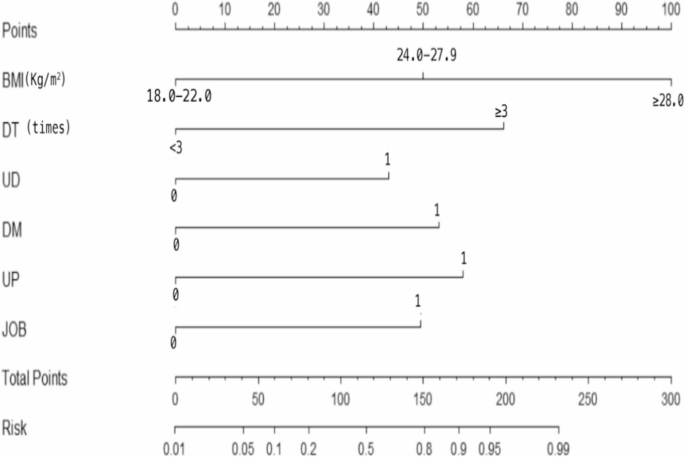
Nomogram for predicting the risk of stress urinary incontinence (SUI) in women. Be aware: To make use of the nomogram: (1) For every predictor variable (e.g., BMI, urethral prolapse), find the affected person’s worth on the corresponding axis; (2) Draw a vertical line upward to the “Factors” axis to find out the rating for every variable; (3) Sum all the person scores to acquire the “Whole Factors”; (4) Draw a vertical line downward from the “Whole Factors” axis to the “Risk of SUI” axis to learn the expected chance of SUI (%).
Model Validation and Analysis: Receiver working attribute (ROC) curves had been plotted for the coaching set (Desk 3) [8], and areas below the ROC curve (AUC) values had been calculated to evaluate model discrimination functionality (Fig. 3). AUC values vary between 0.5 and 1.0, with values nearer to 1.0 indicating superior discriminative potential. The model educated on the coaching set was subsequently utilized to the validation dataset to guage generalizability. Calibration was assessed utilizing the Hosmer–Lemeshow goodness-of-fit check [4, 6, 7], grouping validation samples into ten risk strata and evaluating noticed and predicted constructive case numbers (P > 0.05 indicated good calibration). Calibration curves (Fig. 4) in contrast predicted dangers and noticed outcomes, visualizing model accuracy; ideally, the curve approaches the diagonal line. Resolution curve evaluation (DCA) evaluated scientific utility by calculating web profit throughout numerous threshold chances [8], evaluating intervention choices utilizing the model towards methods of “treating all” or “treating none.” If the model’s web profit curve surpassed each extremes over a broad threshold vary, it demonstrated scientific usefulness. DCA curves had been generated individually for coaching and validation units (Fig. 5). Statistical significance was set at two-sided P < 0.05.



Receiver Working Attribute (ROC) curves for the prediction model of stress urinary incontinence. Be aware: The blue line represents the coaching set, and the orange line represents the validation set. The DeLong check indicated no important distinction between the AUCs of the coaching and validation units (P = 0.208), suggesting that the model has good stability and generalization throughout completely different datasets.

Calibration curves of the prediction model. Be aware: The left panel represents the calibration curve for the coaching set, and the suitable panel represents the calibration curve for the validation set.

Resolution Curve Evaluation (DCA) of the predictive model. Be aware: The left panel represents the choice curve evaluation (DCA) for the coaching set, and the suitable panel represents the DCA for the validation set.
Though this examine offers a promising model, additional exterior validation is required to substantiate its applicability to completely different populations. In future research, we plan to conduct multi-center, potential cohort research with bigger pattern sizes to guage the generalizability and scientific utility of the model throughout various settings and healthcare programs. Exterior validation will probably be important to evaluate the robustness of the nomogram and to refine it for wider scientific use.